Detail at last
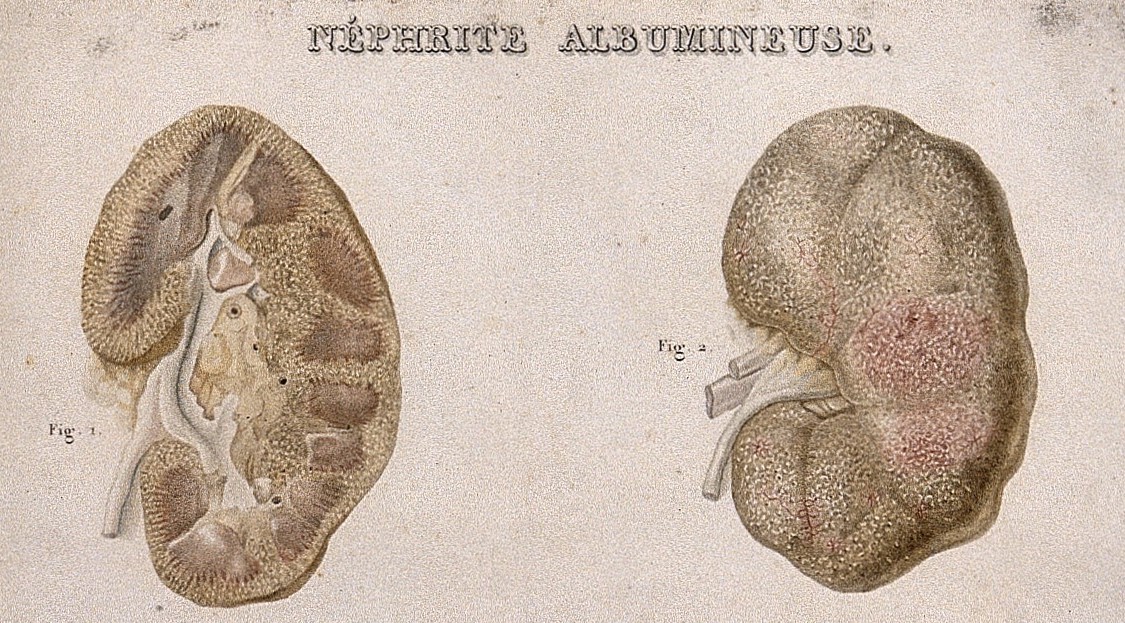 |
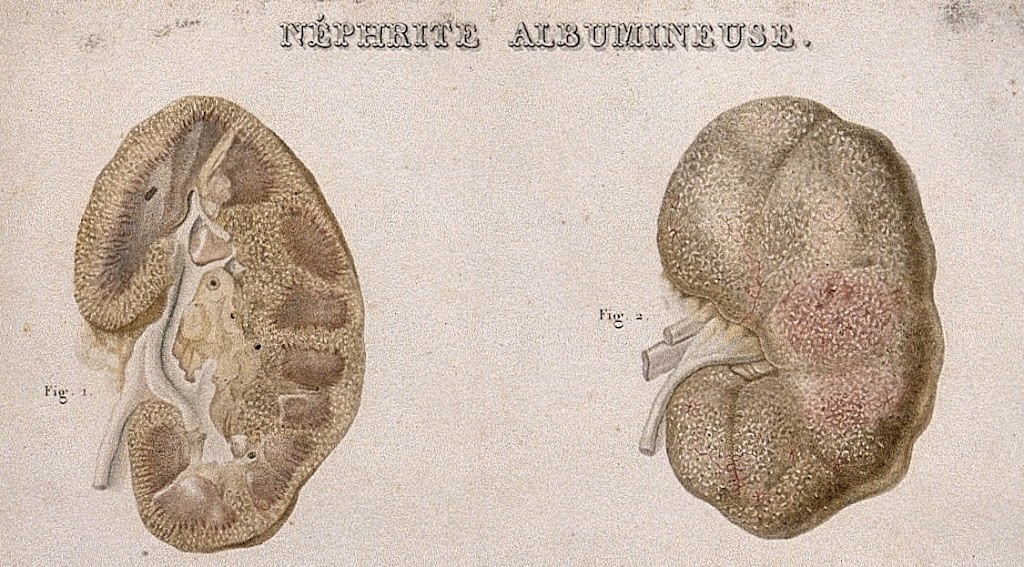
| Ambrose Tardieu for Pierre Rayer (1840) (Wellcome Images V0009820ER) |
For most of the first 100 years of modern nephrology, appearance by eye at autopsy was the closest you could get to seeing the structural detail of kidney disease. But between 1830 and 1870 there were key technical improvements in the quality of microscope lenses, ability to cut thin sections of tissue, and embedding samples in paraffin. Different renal diseases came to be described. By 1914 Volhard and Fahr were able to produce a beautifully illustrated and influential atlas of renal pathology.
Open biopsies
Biopsies were occasionally taken during acute kidney disease, at operations for kidney decapsulation, which were supposed to relieve acute pressure on a swollen kidney. Microscopic examination of diseased kidneys in these circumstances was undertaken from around 1917 in Glasgow, 1923 in Liverpool, and occasionally before that time.
In 1943 Castleman and Smithwick also reported on over 100 kidney biopsies taken during sympathectomy operations for severe high blood pressure. They mostly identified vascular changes.
The first percutaneous biopsies
In 1939 a large series of percutaneous liver biopsies was reported from Denmark. These used a suction technique, using a cutting needle with a syringe on the end, ‘aspiration biopsy’. Kidneys are deeper, smaller, mobile, and have a rich blood supply, but a number of clinicians around the world began to attempt to biopsy them.
Nils Alwall, who independently developed an impressive dialysis machine in Sweden in the 1940s, began to take aspiration biopsies in 1944. One of his patients died, and although he presented his experience at a meeting in 1945, he stopped doing biopsies and didn’t publish his results until 1952. Others were developing the technique independently, notably in Cuba, Senegal, and Italy, as well as in Denmark and the USA.
Acceptance
In 1951 Iversen and Brun reported attempts in 133 patients, getting useful tissue in 66 (50%). However Kark and Muehrcke adopted a modified Vim-Silverman cutting needle and the prone position that we still use now, in place of sitting, and in a flurry of publications 1954-8 reported a much higher success rate and fewer complications. Renal biopsy quickly became an essential technique.
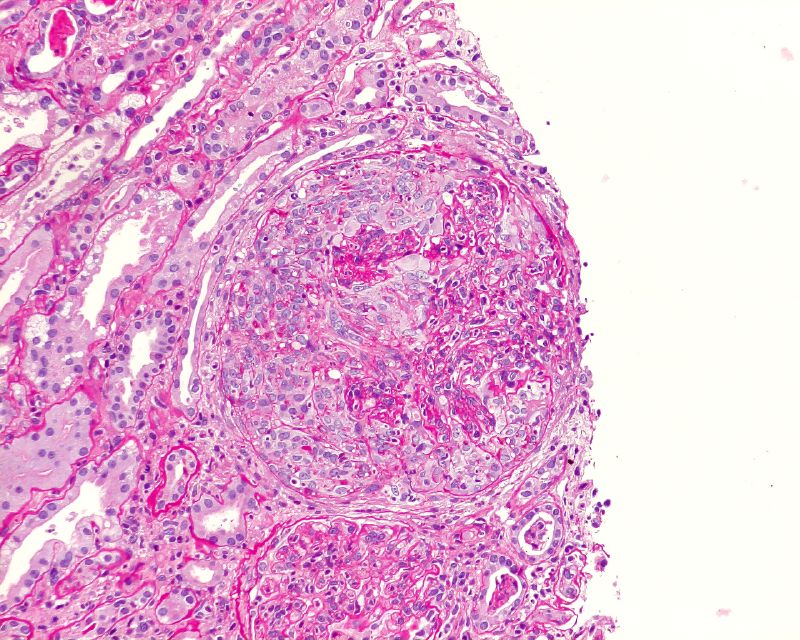 |
| Large cellular crescent in a patient with post-infectious glomerulonephritis; neutrophils visible in glomerular tuft. (Boonyarit Cheunsuchon, Mahidol University, Bangkok (Creative Commons licence) |
In this pre-ultrasound era the kidney was located by anatomical landmarks and plain radiology, and the swing on the needle with respiration when in the kidney; sometimes aided by radiological screening after injection of intravenous contrast medium to outline the kidney.
Dissemination and development
Muehrcke brought his technique to the UK in 1956, visiting the president of the Renal Association Malcolm Milne at Hammersmith Hospital. In his later career he used some of the profits from his Chicago dialysis enterprise to establish an academic renal post at Rush University in Chicago, and to create a scholarship (the Malcolm Milne award) to support visits of young UK nephrologists to US centres.
Immunofluorescence and electron microscopy were first applied to renal biopsies in 1956 and 1957. It became apparent that immunoglobulins were often deposited in glomerulonephritis, and a feast of disease discovery and classification followed. Electron microscopy revealed a key abnormality in ‘minimal change’ disease.
The developments were increasingly discussed by the UK Renal Association, culminating in a landmark meeting of 29 clinicians and pathologists in 1961 at the CIBA Foundation in London. One of the attendees was Robert Heptinstall, who trained in pathology at St Mary’s Hospital in London. In 1966 he published his classic Pathology of the Kidney, the first modern reference book of renal pathology.
Further reading
The discovery of the nephron by Malphigi, Bowman et al 1666-1842 – The glomerulus is a filter (this blog)
Volhard and Fahr – Bright’s disease 100y after Bright (this blog)
Cameron JS, Hicks J. 1997. The introduction of renal biopsy into nephrology from 1901 to 1961: a paradigm of the forming of nephrology by technology. Am J Nephrol. 17:347-58. (paywall)
Weening JJ, JC Jennette. 2012 Historical milestones in renal pathology. Virchows Arch 461:3-11 Authors are pathologists, gives a particularly good account of technical advances, and openly available.
Kark RM, Muehrcke RC. 1954 Biopsy of kidney in prone position. Lancet 1: 1047-9.
D’Agati VD, M Mengel. 2013 The rise of renal pathology in nephrology: structure illuminates function. Am J Kid Dis 16:1016-25.
Wolstenholme GEW, Cameron MP, eds. 1961. Renal biopsy. Clinical and pathological significance. CIBA foundation symposium. London, Churchill. (In US: Ciba Foundation Symposium on Renal Biopsy. Boston, MA: Little, Brown)
Heptinstall RH, 1966. Pathology of the Kidney. Little, Brown and Co. T
Interview with Robert Heptinstall – transcript of an excellent interview.
Arneil GC, Kissane JM, 1987. Was Glasgow first with the kidney biopsy? Pediatr Nephrol 1:381-2 Not quite, but credit due.
Korbet S 2012 Nephrology and the percutaneous renal biopsy: a procedure in jeopardy of being lost along the way. CJASN 7:1545-7
About renal biopsies for patients: From edren from InfoKid (detailed clear info but aimed at parents of children having a biopsy)