The first unequivocally useful drug, 1964
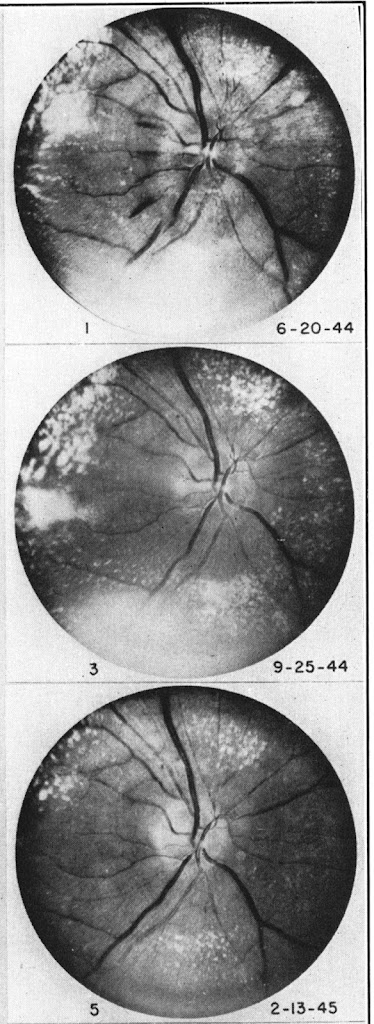
Robust and practical sphygmomanometers (mercury and aneroid) became available in the early 1900s, but regular recording of blood pressure did not become widely routine until the 1920s and 30s. Until then, palpating the pulse offered the only insight, except that ophthalmoscopy could show severe hypertensive retinal changes, neuro-retinitis albuminurica (Figure). The ophthalmoscope had been invented in 1851, but only had electric bulbs after 1900.
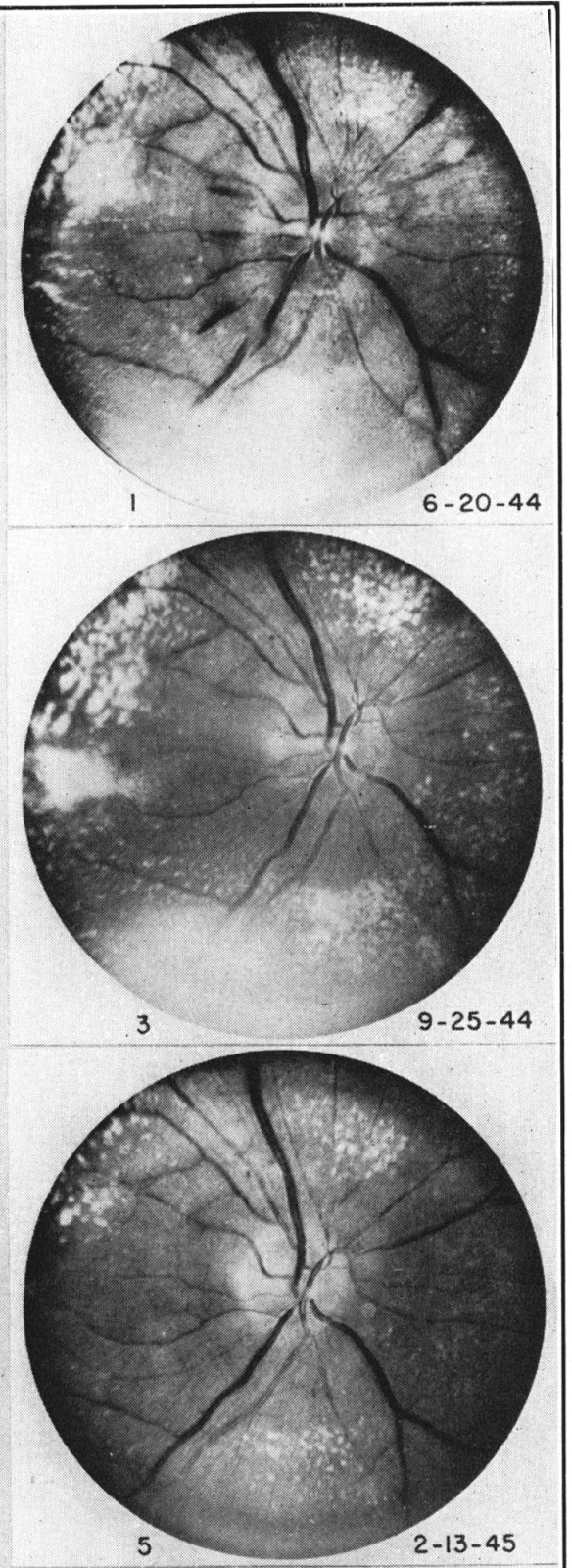 |
| From Kempner 1946 Courtesy of the New York Academy of Medicine Library |
Essential and malignant hypertension
These retinal changes were associated with very high blood pressures and defined Malignant Hypertension (Keith et al 1928). All patients in their series, which excluded those with the syndrome caused by renal disease, died 1-44 months from diagnosis, from cerebral haemorrhage, convulsions, or heart or renal failure.
The term Essential Hypertension was introduced by Erich Frank in 1911 to encompass those who were hypertensive without known cause – and in most patients, without any symptoms or signs. The prognosis was at first uncertain, then controversial, as treatment options were few. But as with proteinuria, life insurance companies led the way in picking up this new measurement.
Essential but not benign
First reports of recordings in those requesting life insurance came from the USA in 1906. As early as 1925, aggregated data from insurance companies were picking up higher mortality in those with high blood pressure, despite disparate methods of measurement and short follow-up.
A 1939 report, covering over 20,000 deaths, found that those with BP >153/>99 had more than four times average mortality. These studies also confirmed that blood pressure values distribute into a smooth curve – there was not a separate group who could be labelled just on numbers as having the disease ‘hypertension’. Mortality risk increased progressively with blood pressure.
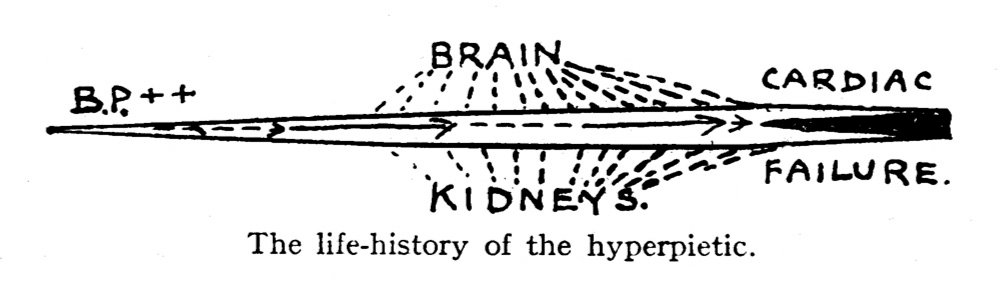 |
| From Hay 1931, courtesy of the British Medical Journal. |
Early treatments
The lack of tolerable treatments was a real barrier to even testing the hypothesis that lowering blood pressure could reduce that risk.
There is some truth in the saying that the greatest danger to a man with a high blood pressure lies in its discovery, because “then some fool is certain to try and reduce it” (John Hay, Professor of Medicine in Liverpool, 1931).
Earliest treatments were rest and sedation. The first partially effective treatment was surgical sympathectomy, cutting sympathetic nerves as they leave the spine, an operation first undertaken in 1923. It was a significant operation and its effects were unpredictable and sometimes slight. These procedures did give pathologists some early kidney biopsies to look at – they showed mostly vascular changes.
Low salt diets had been tested with some success in Paris in 1904, but Kempner’s 1944 Rice and Fruit Diet was widely influential. It included 2,000-2,400 calories from mostly carbohydrate; just 25g of protein, 5g of fat, and only 0.35g of salt. If adhered to, it was often able to lower blood pressure, especially in patients with kidney disease. However patients found it dull, tasteless, and hard to stick to. Others observed that the extremely low salt content was critical, but made adherence difficult.
Some experimental drugs then appeared for those with malignant hypertension. The variable effectiveness of surgical sympathectomy led to the concept of ‘medical sympathectomy’, and work to develop ganglion blockers targeting sympathetic nerves. Hexamethonium was the key development in 1950. These worked in severe hypertension, but were difficult to use and tolerate.
New drugs and clinical trials
The vasodilator Hydralazine, and catecholamine depleting agent Reserpine, were introduced early in the 1950s, but it was the discovery and utility of thiazide diuretics (Chlorothiazide 1958) that opened the door to widespread treatment, as they had fewer side effects. These three drugs were used in the active arms of the first randomized controlled trials in hypertension, the Veterans Administration Cooperative Studies, which commenced in 1964 and reported in 1967 and 1970. Substantial treatment benefits were seen in moderate (diastolic 95-115) as well as in severe (diastolic 115-130) hypertension. Many studies have followed.
Now there is no disagreement about the desirability of lowering higher blood pressures, only over the targets to be aimed for – or perhaps whether there should be fixed targets at all. For those at increased risk of cardiovascular or renal outcomes, usually lower is better, almost regardless of the starting value. But that debate seems likely to continue.
Further reading
Akbar Mahomed produced the first useful clinical blood pressure recordings in the 1870s, and recognised hypertension in patients both with and without renal disease. However his sphygmograph was difficult to use and not suitable for routine use (this blog).
Keith NM, HP Wagener, JW Kernohan 1928. The syndrome of malignant hypertension. Arch Int Med 41:141-88. Classic description of the syndrome.
Kotchen TA 2011. Historical trends and milestones in hypertension research. Hypertension 58:522-538 (open access) Excellent summary of history, research progress, and two-line accounts of key trials.
Freis ED 1995. Historical development of antihypertensive treatment. Ch 164 in Hypertension: Pathophysiology, Diagnosis and Management, eds JH Larach and BM Brenner. 2nd ed. Raven Press, New York. Extended and fascinating account.
Saklayen MG, NV Deshpande 2016. Timeline of history of hypertension treatment. Frontiers in Cardiovascular Medicine (open access). Gives details of key trials.
Kempner W 1946. Some effects of the rice diet treatment of kidney disease and hypertension. Bull N Y Acad Med. 22:358-70 (open access)
Cheatham W 1885. Neuro-retinitis albuminurica. JAMA 6:150-1. Examples of malignant hypertension before blood pressure could be measured.
Hay J 1931. The significance of a raised blood pressure. Br Med J (July 11) 2:43-7. The implications were becoming clear, but gives insight into very limited options available.
Figure 1 shows improvements in the appearance of the retina over 8 months in a patient on Kempner’s rice and fruit diet (Kempner 1946). Courtesy of The New York Academy of Medicine Library.
Figure 2 indicates outcomes of hypertension in the pre-treatment era from Hay 1931. Courtesy of the British Medical Journal.