
A symposium in Edinburgh on 25th March 1961 was one of the first in the UK to consider the full new range of clinical nephrology.
 |
| Twin coil artificial kidney (Kolff-Travenol dialysis machine) in Edinburgh |
Dialysis for acute renal failure (ARF, AKI)
The excitement in the first session is palpable. Nobody at this meeting was negative about the value of dialysis, which was a recent and controversial break from the conservative/dietary management protocols favoured in the UK since 1945. In only two years the number of dialysis centres in the country had risen from 4 to 20. Most had a single machine. Robson in Edinburgh described 60 treated cases. John Merrill, pioneer of dialysis and transplantation in Boston USA, was able to recount 400 (plus 500 treated conservatively), having picked up the potential of dialysis from the Korean War experience with the Kolff-Brigham kidney in 1953.
The UK Renal Association had in 1959 rejected a proposal for a session on dialysis from Dr Frank Parsons, who set up dialysis in Leeds in 1956. Most nephrologists of the time were interested in physiology, not machinery. However such things had begun to be discussed at the first International Society of Nephrology meeting in Evian in April 1960.
What else is new
The new techniques of electron microscopic and immunofluorescence were being applied to human disease, and first observations were described.
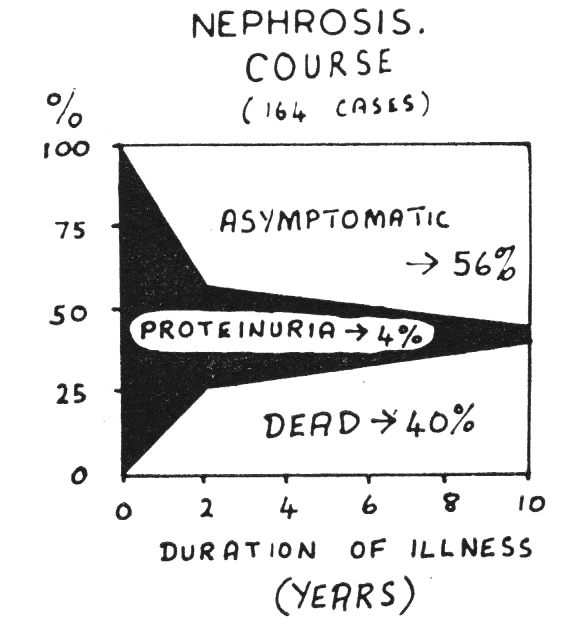 |
| Outcome of nephrotic syndrome in 164 paediatric patients over 30 years. Mortality in the first year was due to infection, later deaths mostly to renal failure. (RCPE, with permission) |
Gavin Arneil from Glasgow presented the outcome of Nephrotic Syndrome in 164 children presenting between 1929 and 1957. Corticosteroids had revolutionised management from 1951. Both their toxicity and the importance of not stopping them too early had been discovered. They reduced deaths from infection, but didn’t prevent renal failure. They had thiazides, but not loop diuretics.
Treatment for end stage renal failure
Attempting dialysis for chronic renal insufficiency was a depressing experience.
“At the present time it is not know whether, given more efficient and practical machines, the life of the patient with chronic renal failure could be sustained indefinitely’ (Robson)
‘In terminal renal disease … haemodialysis … only postpones the evil day and gives false hope to both patient and relatives’ (Parsons)
John Merrill introduced the topic of transplantation, but this had only been successfully achieved in identical twins a dozen times in Boston, and a few months previously the first in the UK. However attempts to prevent rejection of cadaver or live related grafts had very limited success, and that only with whole body irradiation (more on the first transplants). Patients were more likely to die of sepsis than keep their graft, but long term dialysis was not an option.
Not quite. But Belding Scribner had started Clyde Shields on long-term haemodialysis for end stage renal failure in Seattle a year earlier, and presented him in person at the Evian meeting the preceding April, when he had been on treatment for just a month. And at the same time, Roy Calne had just begun the work in Boston that led to azathioprine being tested. That turned out to be the beginning of acceptable success in transplantation too, so that in a few more years, both treatments seemed to be becoming viable.
20 years on
At a similar symposium in 1982, survival by dialysis and transplantation was taken for granted, but poor. For a 50 year-old, 5 year survival was 50%, ‘equivalent to carcinoma of the breast or a heart attack’ (Douglas Briggs, Glasgow). Blood transfusions appeared to lower transplant rejection rates. Azathioprine was the main anti-rejection drug and steroid doses were lower. CAPD was being taken up rapidly, particularly because dialysis capacity was a serious issue in the UK. Cost for an additional year of survival was calculated in the session on ARF.
Types of glomerulonephritis were now well defined, and cyclophosphamide and plasma exchange had become powerful treatments for aggressive glomerulonephritis caused by anti-GBM disease, lupus or vasculitis. A presentation on a new class of anti-hypertensive drug, ACE inhibitors, attracted interest.
Further reading
Symposium. Some Aspects of Renal Disease. Royal College of Physicians of Edinburgh, 1961
Symposium on Renal Disease. Royal College of Physicians of Edinburgh, 1982
Cameron JS. The Early History of the Renal Association. Renal Association History page