Kolff reflects on four available techniques
This fascinating 1947 book of just over 100 pages gives Willem ‘Pim’ Kolff’s own, fuller, more reflective account of the development, testing, and first successful use of haemodialysis. Amazingly, this was achieved while working away from academic centres in Nazi-occupied Holland.
The first 10 pages summarise previous work on developing haemodialysis, and its shortcomings. Then he gives a detailed account of how to make his dialysis machine, including scale technical drawings; and how to gain vascular access (glass cannulas in radial artery and a vein); how to anticoagulate with heparin, and the issues and complications that can arise during a treatment session.
Experiences with Haemodialysis: Patient 17
Most readers will jump to Chapter 4, in which he recounts his experiences with patients. All were at very advanced stages of uraemia, and almost all died, despite temporary improvements in a good number. Then Patient 17, in September 1945, survived. A 67 year old woman with cholecystitis had been anuric for 8 days, was desperately ill and practically comatose. 80 litres of blood were run through the dialyser over 11.5 hours.
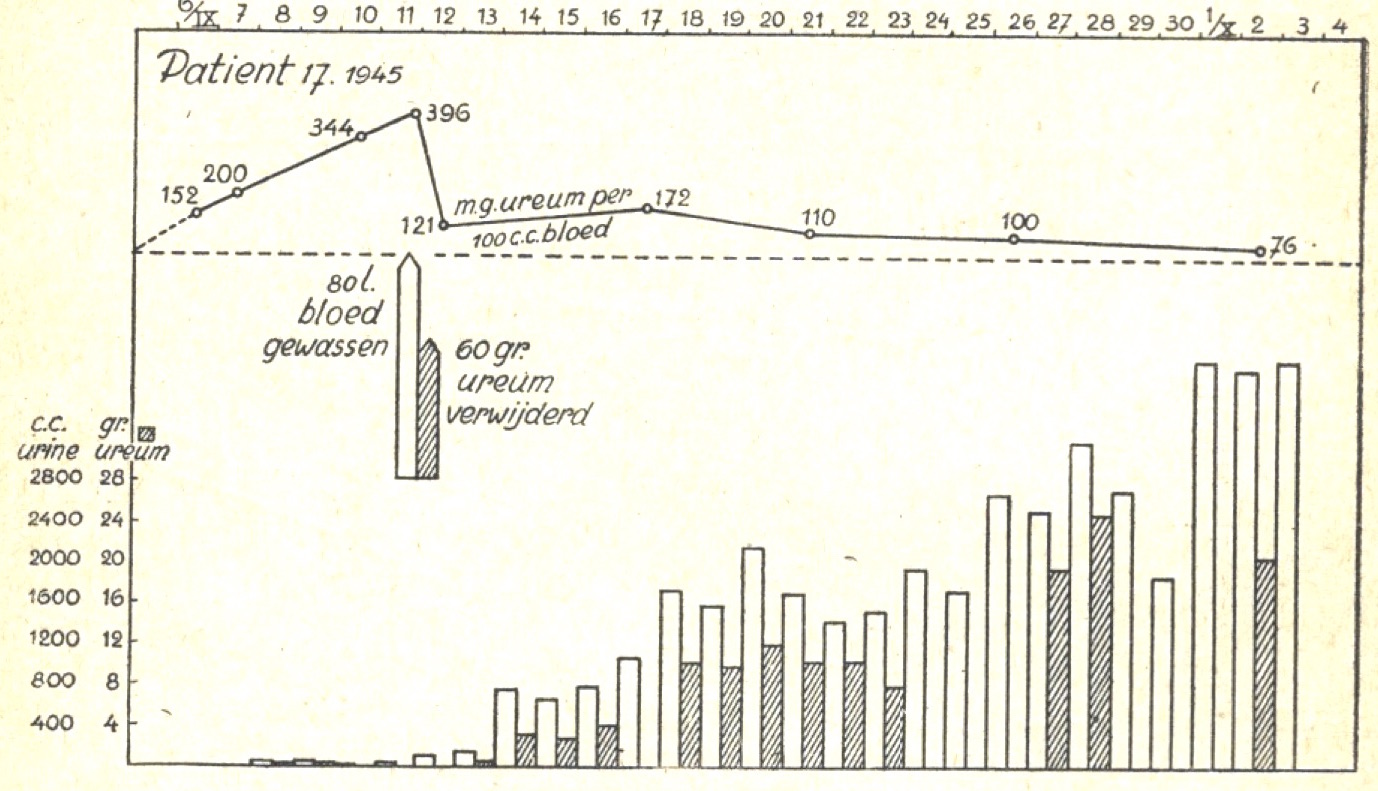
‘During the dialysis her condition was very alarming for some hours, but at the end her general condition was good’.
Blood urea was reduced from 66 mmol/l to 20; and potassium apparently from 14.1 to 4.9.
Pulmonary oedema could be managed by removing blood, and/or by adding more glucose to the bath (dialysate). He distinguished the problems caused by hypertension, which was often very severe, from those due to uraemia. He pointed out that we didn’t know which molecules caused uraemia, but that they were mostly dialyzable.
He proposed dialysis when urea rose above 350 md/dl (58 mmol/l), as he had noted a high risk of sudden death if it rose above 400 (66 mmol/l). He was disdainful of treatments proposed to accelerate kidney recover in acute renal failure, and distinguished cases where dialysis was unlikely to provide lasting benefit.
Peritoneal dialysis
By this time he also had some experience of peritoneal dialysis, then called peritoneal lavage, and in a short Part 2, comments on the successful case published by Frank, Seligman and Fine in 1946. Kolff describes how they replicated this, with two case histories (one recovered), and a table compares the pros and cons of the two techniques which wouldn’t look out of place today.
Intestinal lavage
Limited experience with lavage of a surgically created isolated intestinal loop is described concisely. He pursued this further later. Conceptually it might have created a way to continue dialysis long-term, but inadequate surface areas subsequently proved an insuperable challenge.
Diet and conservative management
Part 4 is just two pages recounting the exciting results being reported at meetings at that stage, not yet published, for conservative dietetic approaches to acute kidney failure.
‘Borst forces patients with severe uraemia to eat 200g of butter and 200g of sugar daily. … The butter and sugar is served in the form of small balls from a refrigerator or is made into a kind of creamy soup, by adding ± 12g of flour and coffee.’
Kolff reported that their own small experience seemed to confirm that maintaining calorie intake could indeed slow down the development of uraemia in an oliguric patient – but that this would not be enough in some cases of acute uraemia. He published their more extended experience 5 years later.
Overview
All of these techniques apart from intestinal dialysis proved useful over the following decades. Nils Alwall in Sweden and Gordon Murray in Canada independently developed their own haemodialysis machines very shortly after Kolff, but haemodialysis was slow to catch on. Other centres found it difficult, expensive, and hard to justify. In the UK, the dietary approach held sway for a decade, while some PD was done, often not in academic centres, and probably under-reported.
The Korean War put haemodialysis back on the map, so that by 1961 a patient with acute uraemia in a good centre would receive conservative management, then possibly either peritoneal dialysis, or increasingly from 1959 onwards, haemodialysis on one of the second generation machines at one of the scarce but growing number of haemodialysis centres.
Further Reading
Kolff WJ. 1947. New ways of treating uraemia. J&A Churchill Ltd, London.
Kolff WJ. 1952. Forced high-caloric, low protein diet and uremia. Am J Med 12:667-79.
Appendix
Some extras from a special copy (Kolff, Thomas Muller, Nathan Levine)