Dropsy becomes treatable in the 1960s
 |
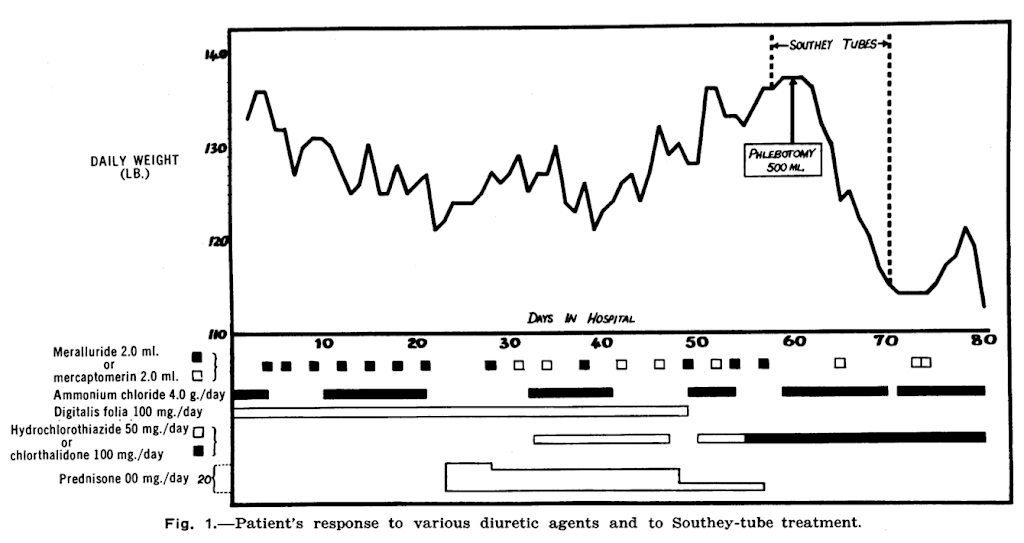
| Failure of pharmacological therapies in a woman with heart failure in 1964, right on the verge of the introduction of loop diuretics. |
During the 1800s it became clear that dropsy (extensive oedema, ascites, pleural effusions) was not a single disease, but a late feature of failure of the heart, liver or kidneys. For around 2,000 years treatment was based on purgatives, bleeding, sweating, and other means to make the body lose fluid.
Physical methods
Heberden (1710-1801) described tapping ascites occasionally, but didn’t find any of the drug therapies consistently effective. Robert Bentley Todd (London, 1809-60) mentioned a technique ‘lately revived on the continent’ of pricking the leg at various points. Southey’s tubes (Reginald Southey 1835-99) developed this technique; silver tubes inserted into oedematous legs allowed fluid to leak out, giving relief of major oedema. The holes left behind often continued to leak, and could become infected. Use of Southey’s tubes continued into the 1960s.
Calomel and inorganic mercury
The remarkable German-Swiss physician Paracelsus (1493-1521) described inorganic mercury-containing compounds as having diuretic properties in 1520. He used Calomel, mercurous chloride, Hg2Cl2. It was more of a laxative than a diuretic, and notably toxic. However in the 17-1800s it was still a standard treatment, often used in combination with the laxative plant extract squills, or (after Withering’s 1775 discovery) digitalis. Calomel was a frequently used drug for William Cullen (Edinburgh) and his pupil Benjamin Rush (Philadelphia).
Organic mercurials, 1920-60
Organic mercury compounds became used to treat syphilis and other infections in the late 1800s. Alfred Vogl, while a medical student in Vienna in 1919, observed a patient with heart failure having a diuresis when treated with with Novasurol. These were weak effects by modern standards, but pharmaceutical companies immediately sought to develop less toxic derivatives. Several, for example Mersalyl (1924), were used for decades. Intravenous use, in particular, was associated with significant toxicity, as the use of calomel had been previously.
The role of salt 1941
Despite 40 years of supportive observations, the central role of salt retention was only fully accepted after Henry Schroeder showed in 1941-2 relief of oedema by limiting salt intake to less than 1g/day in patients with heart failure, and that they had limited ability to excrete higher salt loads. This was strengthened by demonstrations that high blood pressure could be lowered by extreme salt restriction at around the same time. Oral cation exchange resins to bind sodium in the gut had a temporary therapeutic life, but the observations guided pharmaceutical company efforts to develop drugs that caused renal salt loss.
Carbonic anhydrase inhibitors 1937
In 1937 it was noted that the new antibiotic Sulfanilimide caused metabolic acidosis through inhibiting renal carbonic anhydrase – and that it caused diuresis in patients resistant to mercurial compounds. Acetazolamide, introduced in in 1954, was more potent. It retains a few niche indications, including in altitude sickness.
Thiazides 1958
Sharp and Dohme (merged with Merck in 1952) set up a notable renal programme in 1943, aiming to manipulate tubular function pharmaceutically. They produced PAH, probenecid (to preserve penicillin levels in blood), and in 1955 showed that Chlorothiazide increased excretion of sodium and chloride. The drug, marketed in 1958, was a landmark development. Thiazides proved much better at relieving oedema, with few side effects, and they also lowered blood pressure, with randomized BP trials reporting real treatment benefits in 1967 and 1970.
Loop diuretics 1964
The search for more potent compounds in the 1950s led to the discovery of first ethacrynic acid and later furosemide (1959). Furosemide was released in 1964, ethacrynic acid the year after. After 80 years Southey’s tubes began their journey to curious historical artefact.
Potassium sparing diuretics 1961-8
All the new diuretics caused undesirable potassium loss, so there was a search for agents to rectify that, including returning to drugs shelved earlier for the same reason. Spironolactone (1961) and Triamterene (1964) were followed by Amiloride (1968).
The 60s, what a decade
In just one decade, oedema and salt retention became treatable, transforming the care of heart failure, kidney and liver disease, and hypertension, through deliberate manipulation of kidney handling of electrolytes. Dialysis and transplantation came of age in the same decade. Putting humans on the moon was a sideshow.
Further reading
Eknoyan G, 1997. A history of edema and its management. Kidney Int 51 Supp 59:S118-S126. A comprehensive and fascinating account from ancient world to now. Has many further references.
The first effective treatment for a kidney disease was steroids for (some children with) nephrotic syndrome (this blog)
Alfred Vogl – New York Times obituary
Schroeder HA, 1941 (paywall). Studies on congestive heart failure. 1. The importance of restriction of salt as compared to water. Am Heart J 22:141-53. “These studies suggest that restriction of salt is important in the control of the edema of congestive heart failure, but that the restriction of fuids is of little value.“
Anonymous 1951. Oedema and salt. Br Med J 1951 i 1500. Convincing evidence of the value of restricting salt intake to less than 1g per day.
Figures
Walsh AC and Moyes A, 1964. Intractable congestive heart failure successfuly treated with Southey Tubes. Canadian Medical Association Journal 90:1375-6.
Arnold & Sons 1879 Catalogue of surgical instruments. (Entire catalogue from Internet Archive)
One response to “The invention of diuretics”
This was our 50th post. Though a couple weren't really about history, so hold the party.