Low-protein disappoints; attention drawn to proteinuria and blood pressure
The MDRD study was a landmark trial set up to prove the importance of dietary protein in slowing the progression of kidney failure. This had been shown in animal models but human studies were not so clear. It was combined with using two different blood pressure targets, as again these seemed important in animal studies but it was not clear how much we should lower blood pressure in patients.
Patients were recruited from nephrologists and by advertisement; they were known to have a kidney diagnosis. They were not simply people found to have reduced kidney function by random testing. Diabetic nephropathy was excluded but diagnoses were varied. 25% had glomerulonephritis. Almost as many had the genetic condition polycystic kidney disease (PKD, a group you might think whose outcome would not be altered so much by control of diet or blood pressure.
The patients were divided into these groups with higher or lower protein intake, and higher or lower blood pressure:
| Study | GFR | Protein intake | Blood pressure |
| 1 (n = 585) |
25-55 | Usual protein (1.3 g/kg/d) or Low protein (0.58 g/kg/d) |
140/90 or 130/80 |
| 2 (n = 255) |
13-24 | Low protein (0.58 g/kg/d) or Very low (0.28 g/kg/d) |
140/90 or 130/80 |
The very low protein diet was supplemented with essential keto acids and amino acids. Glomerular filtration rate (GFR) was measured every 4 months by iothalamate clearance and normalised for surface area (/1.73m2). Follow up was for an average of 2.2 years.
The Results were surprising
Diet had no impact on rate of loss of GFR or on the number of patients starting dialysis or dying, in either the low or the high GFR groups.
Blood pressure control had no overall effect, but there was a striking benefit from the lower blood pressure target for those with over 1g of proteinuria per day. The benefits increased further as the amount of proteinuria rose.
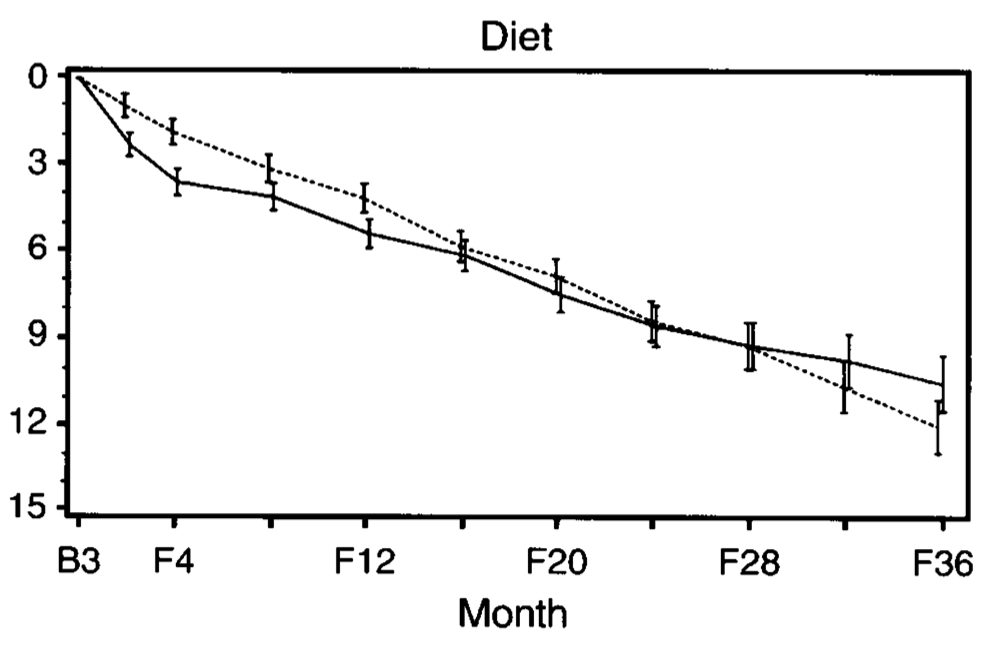 |
| Decline in GFR in study 1. Usual protein group is the dashed line and low-protein the solid line. No significant difference. There was an early fall then slower gradient in the low-protein group but no overall benefit. |
 |
|
Deaths and ESRD in study 2. Very low protein is the solid
line, low protein is the dashed line. Figures from Klahr et
al as below, with permission from NEJM. |
Diet enthusiasts have hoped that there might be a silver lining, but one has not emerged. If there is any long term effect, it seems to be slight. Worse, a 10 year analysis of what happened in the low-GFR group (Study 2) showed that those who had been allocated to the very low protein diet started dialysis no later than the low protein group, but were twice as likely to have died (Menon 2008). The effect seemed to persist long after the study had finished. Surely the last nail in the coffin of very low protein diets, and confirming Thomas Addis’s caution about low protein diets in 1949, ‘We are trying to do something dangerous’.
What else did the trial achieve? Well scores of other studies have come from analysing the details of the rich data collected in the MDRD study. The best known is the MDRD equation, a formula for estimating GFR from serum creatinine which is now in near universal use.
A couple of interesting subgroup analyses were mentioned in the original paper. Patients with polycystic kidney disease did not appear to benefit from blood pressure control. The 53 black patients had a higher rate of loss of GFR than other patients, but it was half the rate in those allocated to the lower blood pressure target group.
Why were the diet results so negative? The conclusion should be qualified: it was not that diet is useless. It was that lowered protein diets are not helpful in well supervised patients with good blood pressure control. Even the higher blood pressure group in MDRD had pretty good blood pressure control. Animals with renal failure probably have comparatively much higher pressures.
How high can protein intake safely be? With those animal experiments in mind, plus a number of concerning anecdotes about the effects of protein supplementation on kidney disease in some individuals, few dare to recommend exceeding ‘moderate’ protein intake.
Personal view: If blood pressure control is poor or supervision difficult, you might argue for lower intakes. If you cannot or do not want to use dialysis to control symptoms in advanced uraemia, targets could be lower still.
Further reading
Diets for chronic uraemia – on this blog
Klahr S et al. The effects of dietary protein restriction and blood-pressure control on the progression of chronic renal disease. New Engl J Med 1994 330:877-84
Menon V et al. Effect of a very low protein diet on outcomes: long-term follow-up of the MDRD study. Am J Kidney Dis 2009 53:208-17.
2 responses to “Surprises from the 1994 Modification of Diet in Renal Disease (MDRD) study”
It's interesting that not a single large, well-conducted diet trial (including Locatelli's 1991 Lancet study) has found a significant protective effect, but meta-analyses that aggregate multiple studies continue to suggest a (modest) benefit. But most studies are small and short, and the funnel plot raises the possibility that negative studies have not been reported. I'm still of the view that there is weak evidence for any benefit from low-protein diet in patients well-treated with ACEi/ARB and good blood pressure targets.
And sometimes wonder heretically how great the symptom-reducing effect is in advanced renal failure too. At that stage people don't have an appetite for much protein anyway.