 |
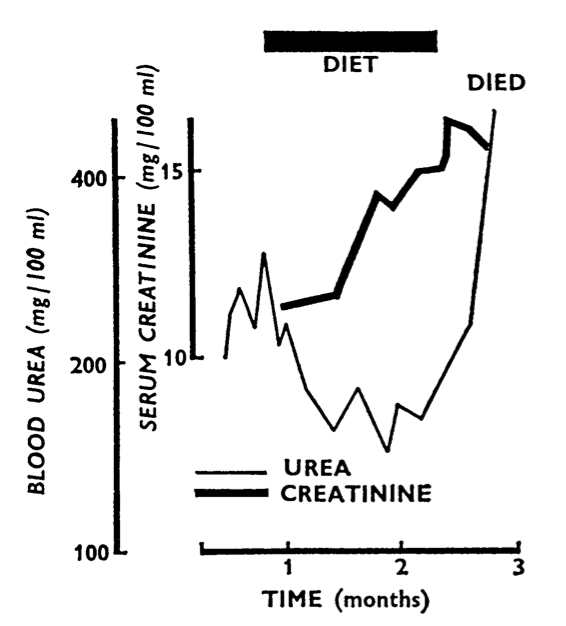
| It didn’t work for her: a 46 year old female patient who stopped
her diet. Note that it was lowering urea but not creatinine.
From Shaw et al 1965, by kind permission of OUP.
|
Low protein diets were shown to prolong the life of uraemic rats in experiments in the 1930s, and it was long held that the products of protein metabolism (which included Urea) were major contributors to the symptoms and signs of uraemia. In the late 1940s, no-protein no-electrolyte diets, the Borst and Bull regimens, were introduced for conservative management of acute renal failure.
Thomas Addis was a strong proponent of low protein intake for chronic uraemia too. In his classic 1949 book Glomerular Nephritis he talked of ‘resting the kidney’, perhaps now interpreted as reducing hyperfiltration, and carefully explained how to achieve it in partnership with patients, dietitians and nurses in the real world. However he also commented
“We are trying to do something dangerous. We are always on the edge of a possible deficiency”.
Referring back to data from the 1920s, when the minimum protein intake compatible with neutral nitrogen (protein) balance was estimated, he prescribed 0.5g of protein per kg weight per day. This was increased by any amount lost in urine, and a bit more was alllowed for growing children. These principles became widely accepted and followed.
Giordano in 1961 was probably the first to advocate a much lower protein intake, 18g, with supplementation of essential amino acids, but this idea became more widely associated with the name of Giovannetti after a 1964 paper in The Lancet. It is interesting that this more extreme management came into vogue just at the time that dialysis and transplantation were beginning to develop. Perhaps there was increased awareness of end stage renal disease, and it was all too obvious who could not be eligible for these new experimental and expensive treatments. The aim was to reduce the symptoms and prolong the life of patients with advanced and terminal uraemia, when symptoms could be severe on more moderate protein restriction.
Giovannetti’s patients were 27-52 years old and had creatinine levels of 900-1600 micromol/l (10-18 mg/dl) on admission. Some of them needed temporary dialysis (the only kind available most likely) to stop vomiting before they could start their diet, but then symptoms improved. The severity of renal failure in their patients is apparent from their report. Two of 8 died but the others remained alive at 10 months.
 |
| The diet |
Attempts to simplify the regimen, and make it more acceptable in the Northern Europe of the time by replacing the starch-based spaghetti with bread recipes designed for patients with phenylketonuria, were described by Berlyne and colleagues in Manchester in 1965. Glomerular filtration rates varied from 1 to 5 ml/min. Those with values greater than 2.5 ml/min tended to do better. They reported lowered urea and phosphate and improved (but persistent) acidosis, and perhaps most importantly, reduced anorexia, nausea and vomiting. In a later paper they also described less drowsiness so that patients tended to die in a bleeding-agitation syndrome, which doesn’t sound such a great success. On this diet death occurred when creatinine was over 1800 micromol/l (20 mg/ml), urea a mean of 80 mmol/l (230 mg/dl) (see Figure). Urea:creatinine levels were generally lower on very low protein diets.
All groups commented on the unpalatability of these diets (click on the diet sheet image to the right) and how difficult patients found it to adhere to them, and to maintain adequate intake, although they seemed to achieve their purpose in the short term.
A number of mostly small and flawed human studies during the 1980s supported that low protein diets reduced the rate of loss of function in patients, a conclusion supported by further animal experiments. However it was not until the Modification of Diet in Renal Disease (MDRD) study in 1994 that the real value of low protein diets in human kidney disease became known. And the answer was not at all what was expected.
Further info
Conservative dietary management from edren (www.edren.org)
Addis T. Glomerular Nephritis. Macmillan (New York) 1949.
Shaw AB, FJ Bazzard, EM Booth, S Nilwarangkur, GM Berlyne. The treatment of chronic renal failure by a modified Giovannetti diet. Quart J Med 1965 34:237-53
Giordano C. Treatment of uraemia using essential amino acid and low protein diets. 1963 Proceedings of the 2nd International Congress of Nephrology 752-7
Giordano C. Protein restriction in chronic renal failure. Kidney Int 1982 22:401-8
Giovannetti S, Q Maggiore. A low-nitrogen diet with proteins of high biological value for severe chronic uraemia. 1964 Lancet 1964 i 1000-1003